Blog

Physiatrists, or rehabilitation physicians, are nerve, muscle, and bone experts who treat injuries or illnesses that affect how you move and function. Physiatrists are medical doctors who have completed training in the medical specialty of physical medicine and rehabilitation (PM&R). Specifically, rehabilitation physicians: Diagnose and treat pain Restore maximum function lost through injury, illness or disabling conditions Treat the whole person, not just the problem area Lead a team of medical professionals Provide non-surgical treatments Explain your medical problems and treatment/prevention plan The job of a rehabilitation physician is to treat any disability resulting from disease or injury, from sore shoulders to spinal cord injuries. The focus is on the development of a comprehensive program for putting the pieces of a person’s life back together after injury or disease – without surgery. Rehabilitation physicians take the time needed to accurately pinpoint the source of an ailment. They then design a treatment plan that can be carried out by the patients themselves or with the help of the rehabilitation physician’s medical team. This medical team might include other physicians and health professionals, such as neurologists, orthopedic surgeons, and physical therapists. By providing an appropriate treatment plan, rehabilitation physicians help patients stay as active as possible at any age. Their broad medical expertise allows them to treat disabling conditions throughout a person’s lifetime.

The Healing Art of Jin Shin Jyutsu The body contains energy pathways that feed life into all of the cells. When one or more of these pathways become blocked, the effect can lead to discomfort, pain, illness and injury. Jin Shin Jyutsu (pronounced Gin Shin Jitsu) a Japanese form of acupressure, helps release the tensions that cause these various physical symptoms. By gently applying the hands to a clients’ fully clothed body, Jin Shin Jyutsu re-harmonizes and balances the energy flows. This aids in healing, promotes optimal health and helps the client to feel better. The practice of Jin Shin Jyutsu naturally addresses any latent emotions which could be hindering physical healing. Self-care is a beautiful piece of Jin Shin Jyutsu. By developing an awareness of the life force within yourself, you can learn to harmonize your mind, body & spirit. Your hands are your jumper cables and by holding your fingers, toes or utilizing simple flows you can easily become more responsible and engaged in maintaining your own health, balance and happiness. For example, if you have a stomach-ache or are overcome by worry hold your thumb and breathe deeply. Both symptoms will melt away. This article was written by Beth Lendrum, Holistic Health Counselor, Jin Shin Jyutsu Practitioner 916-467-6232 bethjsj@gmail.com Beth Lendrum has studied many different healing modalities in her journey to help others. These modalities include Reiki I, Eastern nutrition, Chinese Medicine, Massage Therapy, essential oils and Jin Shin Jyutsu. Once she discovered Jin Shin Jyutsu in 2004, she knew that practicing this was her calling. She studied Eastern nutrition and Chinese Medicine in a Traditional Chinese Medicine Hospital in Beijing China. In 2007, she travelled to Japan to study with the last living Jin Shin Jyutsu master. Beth lives in El Dorado Hills with her husband, 2 children and her healing miniature poodle, Cisco. Beth has a practice in El Dorado Hills and Roseville. Beth Lendrum is not affliated with the Spine & Nerve Diagnostic Center but has helped treat patients referred to her by the providers at Spine & Nerve Diagnostic Center.

The University of Nottingham located in the United Kingdom published a study in 2008 which looked at the role that the length of people’s fingers may play in predicting osteoarthritis. The researchers at the University of Nottingham studied more than 2,000 people. The conclusion of the study was that people who have an index finger shorter than the ring finger are up to twice as likely to suffer from osteoarthritis. Osteoarthritis is a general term, which refers to degeneration of joint cartilage or the bone. This is most commonly associated with age, but some people develop it at an earlier age than others. This study seems to conclude that people who have a longer ring finger than index finger have a higher rate of developing osteoarthritis earlier than one would expect. A more recent study published in March 2014 reported in the Oxford University Press demonstrated the same thing. In the Oxford University study published in the Journal of Rheumatology, they specifically looked at osteoarthritis of the knee and found that the lower the ratio of the second digit length to the fourth digit length, the higher the incidence of osteoarthritis in the knee and higher the need for a total hip replacement. The second study looked at 580 people and followed them over a 10.5 year period. Interestingly, the ratio of the second digit to the fourth digit has hormonal connections. The amount of prenatal testosterone levels seems to account for having a fourth digit that is taller than one would expect. Other prenatal factors that effect the digit ratio are lower estrogen concentrations. Men typically have shorter second than fourth digits, and in women, the fingers tend to be equal in length. Based on these studies, we can draw the conclusion that men probably have a higher risk of osteoarthritis than women; and that among both men and women, the ratio of the fourth digit to the second digit can be one predictor of osteoarthritis. However, this is only one factor, and components such as other genetics, family history, injuries and type of work are also contributors to osteoarthritis.

DEA Reclassifies Hydrocodone Combination Products to Schedule II On August 22, 2014, the U. S. Drug Enforcement Administration (DEA) published the Final Rule moving hydrocodone combination products (HCPs) from Schedule III to the more-restrictive Schedule II classification. The Final Rule in effective October 6, 2014. The Controlled Substances Act (CSA) places substances with accepted medical uses into one of four schedules, with the substances with the highest potential for harm and abuse being placed in Schedule II, and substances with progressively less potential for harm and abuse being placed in Schedules III through V. Schedule I is reserved for those controlled substances with no currently accepted medical use and lack of accepted safety for use. Hydrocodone combination products (HCPs) are drugs that contain both hydrocodone, which by itself is a Schedule II drug, and specified amounts of other substances, such as acetaminophen or aspirin. Hydrocodone combination products include Vicodin, Norco, Lortab, Lorcet, and Vicoprofen. The Final Rule was made to address concerns about the abuse potential of HCPs. The Centers for Disease Control report that drug overdose is the leading cause of injury death. More than 16,000 people die each year from pharmaceutical related death in the U.S. Hydrocodone is the most prescribed drug in the U.S. Americans consume 80 percent of the world’s supply of narcotics but only account for 4.6% of the world’s population. What does this mean to patients who are prescribed hydrocodone? Doctors can no longer call in or fax prescriptions for HCPs. Prescribers will need to prepare HCP prescriptions on hard-copy, tamper-resistant prescription forms, for patients to bring to their pharmacy. Only a 30 day supply can be written. Refills are not allowed unless the patient is evaluated by a health care provider and then written by the provider.

An estimated 116 million adults experience chronic pain, according to a report published by the Institute of Medicine of the National Academies, and treatment is all too often “delayed, inaccessible, or inadequate…” according to committee chair Dr. Philip Pizzo of the Stanford University School of Medicine, who co-authored the report. The Academies’ report, Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research acknowledges that pain is more than just a physical symptom, and is not always resolved by curing the underlying disease. Chronic pain –defined as pain lasting longer than 12 weeks—is individual and “a disease in its own right;” managing it successfully requires an individualized approach that addresses all the factors that influence pain. A review published in the journal Anesthesiology found that people who try to ignore their long-term pain may ultimately hurt more. Dr. Teresa Long, Director of the Persistent Pain Management clinic at the University of Kansas Hospital explains: “Left untreated, chronic pain often gets worse over time; the nerve pathways become more sensitive and pain sensations escalate. After a while, the feeling can end up lingering even after the actual tissue or bone has healed.” Such is the case with Reflex Sympathetic Dystrophy, or RSD, a neuropathic pain disorder in which pain from one area spreads to other parts of the body. One patient from the Spine & Nerve Center with RSD has trouble with his memory and sleeps only two to four hours each night. He had to retire early from his career because of the physical labor involved, and due to his need for pain medication, he can’t apply for even a very simple day job because he wouldn’t be able to pass the drug test. There is no cure at this point for RSD; one can only manage the pain. He reported feeling like his “life was over” and received little sympathy because, for several years leading up to the diagnosis, others could not be convinced that he was in pain. Another Spine & Nerve patient, Venus Furtado, was diagnosed with Fibromyalgia – a nerve disorder characterized by widespread pain and fatigue— five years after she was involved in a serious car accident. She’s been living with chronic pain since 1990. When you have Fibromyalgia,” she said, “taking a shower can feel like being hit with ten thousand baseball bats.” Even wearing loose clothing can be painful some days. Ms. Furtado had to make wholesale life changes to accommodate her pain; she was unable to continue her career as an alcohol and drug counselor because of the mental fog that accompanies fibromyalgia (often called “Fibro-fog”). There is little relief from the pain. “Even when you’re asleep,” she said, “the body is always fighting the pain, and you wake up exhausted.” Chronic pain’s lack of visibility often compounds the physical struggle. People suffering from chronic pain aren’t necessarily in a wheelchair or on crutches, so others don’t always sympathize or take their pain seriously. The US Pain Foundation created an organization to help counter this problem; the INvisible Project helps builds community among chronic pain sufferers and educates the public through stories and photography. It shows that the pain is real, even though you can’t see it. We at the Spine & Nerve Center invite you to participate, and more details are available here: www.invisibleproject.org . For more information on chronic pain, please see the National Institute of Health’s fact sheet: http://www.ninds.nih.gov/disorders/chronic_pain/detail_chronic_pain.htm and speak with your physician about effective pain management.

Most people in the Western world will suffer from disruptive lower back pain at some point in their lives. And studies show that about 75% of people who’ve had one bout of debilitating back pain will have another within a year, which often leads to a downward spiral of pain and a weakening in the muscles of the lower back. But there’s good news: even if you have back pain now, a commitment to the right kind of exercise will help keep future back pain at bay, according to a broad new review published in the Journal of American Medicine Association, Internal Medicine . This comprehensive, high-quality study involved more than 30,000 participants with back pain, and systematically evaluated a range of back pain prevention tactics to determine what really works and what doesn’t. Several key prevention methods were evaluated: shoe orthotics, back belts, a variety of different exercise programs, education about lifestyle changes, and exercise programs that also included some education about back-pain prevention. The study defined a successful prevention program as “one that had kept someone from reporting another bout of back pain within a year or longer, or that had staved off lost work time due to back problems.” The study’s conclusion was surprising: education, back belts, and orthotics were almost totally ineffective without exercise. Heat therapy, massage, and other passive treatments without exercise were equally inconclusive in their effectiveness. It was only the exercise programs – alone, or with education about lifestyle changes – that proved their mettle in this vast and rigorous study. Exercise with education reduced the incidence of another episode of back pain in the following year by 45 percent, or almost half. Further, the type of exercise regimen didn’t much matter. Whether the program focused on strengthening the core and back muscles, or whether it combined aerobic conditioning with strength and balance training, as long as the person exercised regularly, —that is, two to three sessions per week, every week—their chance of low back pain recurrence was significantly reduced. It’s possible that one type of exercise program is better than others, but this particular study didn’t focus on evaluating types of exercise regimens in great detail. The important takeaway from this groundbreaking study is that for most people, it is within your power to keep the low back strong. The team that conducted this research intends to mount future studies that would compare different routines and follow participants for several years, to determine the long-term benefits of the various fitness programs. Before you dive into a back-strengthening workout, your health professional should determine that you have no serious injuries and each of these movements is safe for you. Then try this menu of exercises, designed by a Certified Strength and Conditioning Specialist to prevent and treat lower-back pain: Eight Moves to Boost Back Resiliency

Morphine Equivalent Dose (MED), also known as Morphine Milligram Equivalents (MME) is a numerical way to compare different opioids (narcotics). For example, if person A is on 4 tablets of Norco (hydrocodone/acetaminophen) 10/325 and person B is on 4 tablets of Percocet (oxycodone/acetaminophen) 10/325, how do we know who is on a higher dose? We can calculate the MEDs. 1mg of Hydrocodone has an MED of 1, whereas 1 mg of Oxycodone has an MED of 1.5. Therefore, person A is on 40 MEDs per day and person B is on 60 MEDs per day. If person C is on 20 mg of oxycontin (oxycodone ER) twice a day and taking 4 Norco, then the total MED is 100. Why is this important? It is important because opioids are always associated with a risk of overdose and death. Higher doses of opioids are also associated with lower rates of return to work and higher rates of emergency room visits. People with total MEDs greater than 50 (5 Norco per day) have a 2 fold increased risk of overdose compared to people with MEDs lower than 20 (2 norco a day). People with MEDs of 100 or higher have a 9 fold increased risk of overdose. A 2016 study published in The Journal of Addictive Disorders (J Addict Dis. 2016 ; 35(1): 42–51. doi:10.1080/10550887.2016.1107264) found that most patients on opioids under-estimated their risk of overdose. Knowing you MED will help you understand your risk and may save your life! A chart to calculate MED is available from the Centers for Disease Control and Prevention at https://www.cdc.gov/drugoverdose/pdf/calculating_total_daily_dose-a.pdf

For years we have known that opioids (drugs such as Norco, percocet, oxycontin, morphine, fentanyl, etc.) are dangerous. They can lead to dependence and addiction. They can often also lead to overdose and death. A new study suggests that the risk is higher than previously thought. A Centers for Disease Control and Prevention (CDC) study, released on March 17, 2017, (https://www.cdc.gov/mmwr/volumes/66/wr/mm6610a1.htm) evaluated the likelihood of long term opioid use by studying opioid use patterns in the U.S. between 2006-2015. The study demonstrated that patients who had one day of opioid therapy had a 6% chance of long term dependence (still being on it one year later). People who took opioids for eight days or longer had a 13.5% chance of still being on them one year later. And people who used opioids for 31 days or longer had a 29.9% chance of being on them one year later. The CDC study’s conclusion was as follows: “When initiating opioids, caution should be exercised when prescribing >1 week of opioids or when authorizing a refill or a second opioid prescription because these actions approximately double the chances of use 1 year later.” Because of these risks, we will try to prescribe the lowest dose of opioid (narcotic) that is helpful to reduce your pain. In some instances, we will decide against opioids to treat your pain as the risk outweighs the benefits.

Please click on this link for this article by Pauline Bartolone. Drug Overdose Deaths Plateau In California, Soar Nationally This story was produced by Kaiser Health News , which publishes California Healthline, an editorially independent service of the California Health Care Foundation.

I recently reviewed a report on acupuncture for chronic pain. It reviewed 13 clinical randomized trials that occurred up until December 2015 and included over 20,000 patients. It compared the use of acupuncture to no acupuncture in patients or sham acupuncture, which was fake acupuncture and it found a significant difference in both pain relief and improved function in the patients using real acupuncture. It also found that the results can persist over many months. Our clinic does feel that acupuncture can be a significant beneficial modality for treatment of many types of pain. Patients can sometimes lower their pain medication with the use of acupuncture. Some insurances do cover it. If you would like to discuss this with your provider let us know.

What are the Genicular Nerves? The genicular nerves are small sensory nerves around the knee that carry pain signals from the knee joint to the brain. For patients with chronic knee pain—often from arthritis or after knee surgery—treating these nerves can reduce pain and improve function. What is a Genicular Nerve Block? A genicular nerve block is a diagnostic procedure in which a small amount of numbing medication (local anesthetic) is injected near the genicular nerves. Purpose: To determine if these nerves are contributing to your knee pain. What to expect: If your pain improves significantly after the injection, you may be a good candidate for a longer-lasting treatment called radiofrequency ablation (RFA). What is Radiofrequency Ablation (RFA)? Radiofrequency ablation uses a special needle to apply heat to the genicular nerves, interrupting their ability to send pain signals. Goal: Provide longer-lasting pain relief compared to a nerve block alone. Duration of relief: Many patients experience relief for 6–12 months or longer. The nerves may regenerate over time, and the procedure can be repeated if needed. Who is this for? Patients with chronic knee pain that has not improved with medications, physical therapy, or injections. Patients with knee arthritis who are not ready or not candidates for knee replacement surgery. Patients with persistent pain after knee surgery. How is the Procedure Done? You will lie comfortably on a procedure table. The skin over your knee will be cleaned and numbed with local anesthetic. Using X-ray or ultrasound guidance, the physician places thin needles near the target nerves. For a nerve block, numbing medicine is injected. For RFA, after numbing, the physician uses radiofrequency energy through the needle to heat the nerve tip and reduce pain signal transmission. The procedure usually takes 20–40 minutes. After the Procedure You may feel soreness at the injection site for a few days. Pain relief may be gradual, taking a few weeks after RFA. Activity is generally light for the first 24 hours, then you may resume normal activities. Expected Results Many patients report significant reduction in knee pain, improved mobility, and better quality of life. The effect is temporary but often long-lasting. If pain returns, the procedure can be repeated. Risks (Uncommon) Temporary soreness or bruising at the injection site Rare infection or bleeding Nerve irritation or temporary numbness
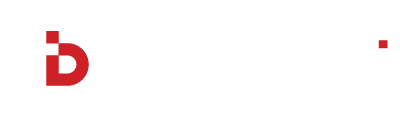
Understanding Basivertebral Nerve Ablation (Intracept) for Chronic Low Back Pain Chronic low back pain is one of the most common complaints among patients, affecting quality of life, mobility, and even mental well-being. While there are many causes of low back pain, one source that's often overlooked is vertebrogenic pain—pain originating from the vertebral endplates. Basivertebral nerve ablation, also known as the Intracept procedure, is an innovative, minimally invasive treatment specifically designed to target this type of pain at its source. What is Vertebrogenic Pain? Vertebrogenic pain occurs when the vertebral endplates—where the vertebrae connect to the spinal discs—become damaged or inflamed. This can lead to chronic pain that’s resistant to traditional therapies like physical therapy, medications, and even other types of spinal injections. For years, there weren't many effective treatments for vertebrogenic pain. But recent advancements in medical technology have led to the development of the Intracept procedure. What is the Intracept Procedure? The Intracept procedure is a minimally invasive treatment that targets the basivertebral nerve, which transmits pain signals from the vertebral endplates. By ablating, or "turning off," this nerve, the Intracept procedure disrupts the pain pathway, providing significant and lasting relief for many patients. How Does It Work? During the procedure, a specialized probe is inserted into the vertebra through a small incision. Using radiofrequency energy, the probe heats and ablates the basivertebral nerve, effectively "shutting down" the pain signal being sent from the damaged vertebra. The entire procedure typically takes about an hour and is performed on an outpatient basis, meaning most patients can go home the same day. Who is a Candidate? The Intracept procedure is intended for patients who: Have been experiencing chronic low back pain for more than six months. Have not found relief from conservative treatments like physical therapy, medications, or injections. Have MRI findings that indicate Modic changes, a marker of inflammation and degeneration in the vertebral endplates. Do not have significant disc or nerve compression that would otherwise explain their pain. Benefits of Basivertebral Nerve Ablation Long-Lasting Pain Relief : Many patients experience significant pain reduction that lasts years after the procedure . Minimally Invasive : This outpatient procedure requires only a small incision, leading to quicker recovery times compared to traditional back surgeries. Improved Quality of Life : By targeting the nerve responsible for vertebrogenic pain, the Intracept procedure can restore function and improve quality of life. What to Expect After the Procedure Recovery time varies, but most patients can return to normal activities within a few days. You may experience some soreness at the treatment site, but this typically resolves quickly. Patients often report gradual improvement in their pain levels over several weeks, with the best results seen at the 3- to 6-month mark. Is Intracept Right for You? If you’ve been dealing with chronic low back pain that hasn’t responded to other treatments, and if MRI findings suggest Modic changes in your vertebrae, the Intracept procedure may be worth considering. It’s important to consult with a specialist who can evaluate your unique situation and help determine if basivertebral nerve ablation is the right option for you. Final Thoughts At Spine & Nerve, we’re committed to providing innovative, evidence-based treatments to help our patients find relief and improve their quality of life. The Intracept procedure is a promising solution for those suffering from vertebrogenic pain, offering an option where traditional therapies may fall short. If you’re ready to explore whether basivertebral nerve ablation could be the answer to your chronic low back pain, reach out to our team to schedule a consultation. Together, we’ll work to find the best treatment plan to get you back to living your life, pain-free.

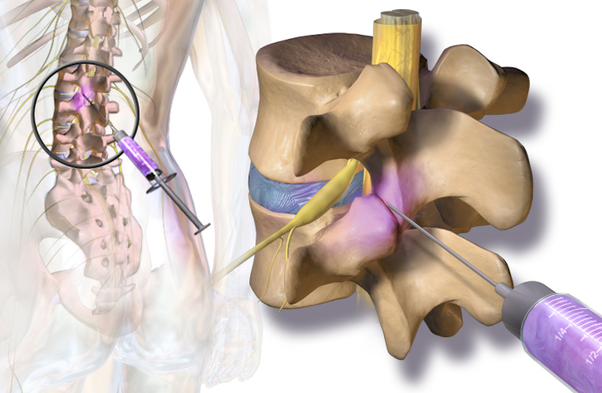
A sacroiliac joint (SI) injection is an image guided, minimally invasive method of targeted drug therapy which is performed to relieve low back/buttock pain. Steroid medication can reduce the swelling and inflammation caused by conditions such as arthritis or joint dysfunction. This minimizes side effects when compared to oral medications and increases efficacy. How is a sacroiliac joint injection performed? Patient Positioning The patient lies face down. Tissue Anesthetized A local anesthetic (typically lidocaine) is used to numb the skin and the tissues along the anticipated path of the needle. Fluoroscopic Guidance Using a fluoroscope for guidance (live x-ray guidance), the physician directs the needle toward the sacroiliac joint. A contrast solution is injected to assess for ideal location and safety. The physician uses the fluoroscope to confirm the correct location of the needle tip. Steroids Injected A steroid-anesthetics mix is injected into the sacroiliac joint, bathing the painful tissues with a potent anti-inflammatory medication. End of Procedure The needle is removed and a small bandage is applied to cover the tiny needle surface wound. How long does it take for the sacroiliac joint injection to work? Most people feel some benefit from the injection between 3-7 days however it can take up to two weeks before we see the full results. Who performs a sacroiliac joint injection? Sacroiliac joint injections are performed by one of the board certified interventionalists at Spine & Nerve Diagnostic Center (SNDC). Our interventionalists have performed thousands of these procedures. Where are sacroiliac joint injections performed? Sacroiliac joint injections are typically performed at our state of the art SNDC procedure suites.

Overview: Whiplash happens when your neck jerks back and forth quickly and violently, causing your spine to bend past its normal range of motion. This can injure the vertebrae of your cervical spine and/or the ligaments and muscles in your neck. Causes: Whiplash is commonly caused by rear-end collision motor vehicle accidents or by contact sports such as football. Symptoms: You may feel pain and stiffness in your neck, shoulders, back, and arms at the time of your injury, or it may begin days later. Treatment Options: Treatment options may include rest, physical therapy, medications and injections.
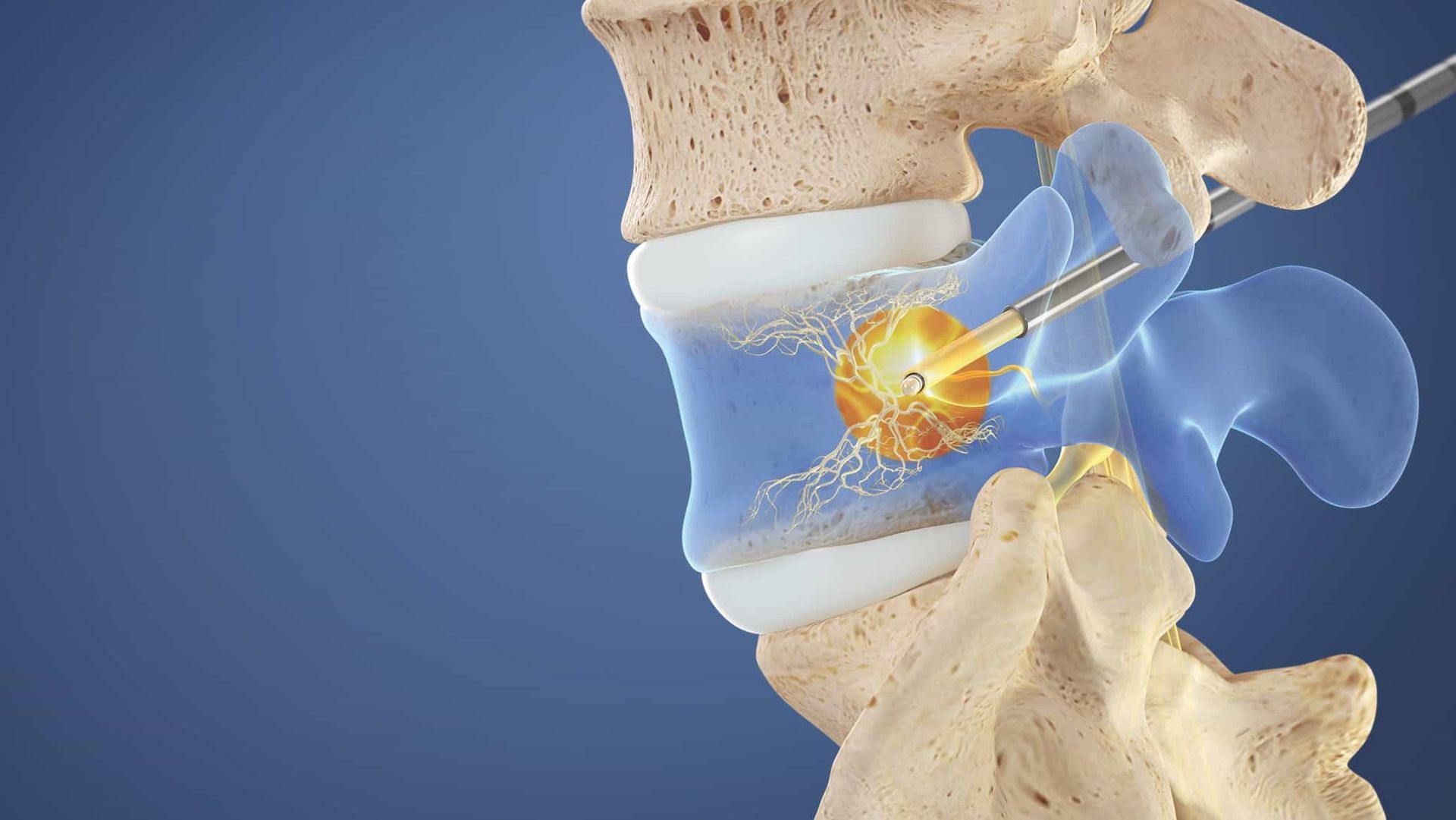
Overview The rotator cuff of the shoulder is composed of four different muscles that support the shoulder joint. This group of muscles keeps the head of the humerus (upper arm bone) secured within the shallow socket of the shoulder joint. When the rotator cuff tendons are injured they become irritated or damaged, resulting in pain, weakness and reduced range of motion. Rotator cuff injuries are common and increase with age, in people who have jobs with overhead motions such as painters and carpenters. Many people can manage their symptoms and return to activities with physical therapy to improve strength and flexibility; however some patients also require surgical interventions to help correct the injury. Symptoms Rotator cuff injuries can manifest as pain, weakness, and/or range of motion. Pain in rotator cuff injuries can be described as a deep ache in the shoulder that can also disturb sleep. Rotator cuff injuries will make it difficult for the person to perform any over head motions such as brushing your hair, or reaching behind your back. Patients may also experience weakness when performing specific movements. Diagnosis Diagnosis of rotator cuff injuries is primarily through physical exam with your medical provider. X-rays, ultrasound, and MRI are also utilized to help diagnose the extent of rotator cuff injuries. Treatment Conservative treatments for rotator cuff injuries include rest, ice, and physical therapy. If these do not provide relief then cortisone or steroid injection can be helpful in reducing inflammation in the shoulder joint. As a last resort corrective surgery may be needed to repair the rotator cuff tendons, this is typically done arthroscopically.

Overview Knee osteoarthritis is a degenerative disease involving the cartilage in the knee joint. Osteoarthritis occurs when the protective cartilage surrounding the end of your bone begins to wear down. It can most commonly affect the knees, hips, hands, and spine. Symptoms can usually be managed, but the damage to the joints can never be reversed. Risk factors for developing osteoarthritis include age, gender, obesity, previous joint injuries, repetitive stress on a joint, genetics, bone deformities, and metabolic disorders. Symptoms Symptoms of osteoarthritis develop slowly over time and can vary from person to person. Most commonly, patients will experience joint pain, stiffness (especially in the morning), tenderness around the joint, loss of flexibility or range of motion, grinding sensation, and swelling. Diagnosis Diagnosis of osteoarthritis of a joint can be made by taking an x-ray of the joint to evaluate the bones in the knee joint. An MRI may also be useful in diagnosing osteoarthritis to help evaluate the soft tissue around the joint. Treatment Treatment of osteoarthritis first begins with lifestyle changes including consistent exercise and proper weight management. Physical therapy, and pool therapy have also been shown to be effective in helping treat osteoarthritis pain. Additionally, alternative movement therapies such as tai-chi and yoga have been found to help reduce pain caused by osteoarthritis. Traditional medication options include acetaminophen (Tylenol), and non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen, or Aleve. Supplements such as glucosamine/chondroitin, capsaicin, and omega-3 fatty acids, while controversial in efficacy, have anecdotally reduced patient’s osteoarthritis pain. Devices such as knee braces and a TENS unit can also provide relief. Typically, if lifestyle changes, therapies, and medications fail to relieve pain, then cortisone or steroid injections can be performed to help reduce inflammation in the knee joint. Other available injections include hyaluronic acid, prolo injection therapy, and platelet-rich-plasma injections. Finally, if all conservative measures fail, the patient can undergo surgery to change the structure of the knee. Two types of surgeries are available: partial knee replacement and total knee replacement.
This is a disease of the spine indicating degenerative changes, sometimes referred to as arthritis of the spine. It can happen at any level (cervical, thoracic or lumbar) and results in different types of pain including mechanical and radicular pain. CAUSES Primarily this is caused by aging and normal wear and tear. With time, the components of the spine, including the vertebrae, the discs between the vertebrae, and the joints of the spine rub against one another, causing pain. SYMPTOMS Cervical Spine: neck, shoulder and arm pain. Radicular symptoms may occur including numbness, weakness in the arms or legs. Thoracic Spine: upper chest and abdomen pain, and may cause numbness, tingling and weakness in the legs Lumbar Spine: lower back, buttocks, and leg pain; and may cause numbness, tingling and weakness in the lower leg. This is often times worsened with sitting, twisting, lifting and bending. TREATMENT This varies based on severity of degeneration, and symptoms patients describe. It includes anti- inflammatory medications, physical therapy, water therapy, back braces, spinal injections and in severe cases, surgery.
Facet joints are found on the back of the entire spine (cervical, thoracic and lumbar). Each vertebrae rests on top of one another at these facet joints. These joints may become inflamed or irritated, causing pain. A steroid injection into the joint may be used to help alleviate pain and diagnose the source of a patient’s pain. Q&A 1. How is a facet joint injection performed? a. Patient positioning: face down on a procedure table. 2. Will the procedure be painful? a. A local anesthetic is used to numb the skin. This feels similar to a bee sting and lasts for a very short time, usually less than 30 seconds. 3. How does the physician know where to inject? a. The physician uses fluoroscopic guidance (live XR imaging) directing the needle into the facet joint space. A contrast solution is injected and confirms the location of the medication to be placed. 4. What is injected? a. A mixture of anesthetic (numbing medicine) and steroid (anti-inflammatory) is injected into the joint space. 5. End of Procedure a. The needle is removed and a small bandage is placed to cover the site of the injection. 6. How long will it take to work? a. Relief usually takes 3-7 days to estimate relief. 7. Who performs a facet joint injection? a. Facet joint injections are performed by one of the board certified interventionalists at Spine and Nerve Diagnostic Center (SNDC). Our interventionalists have performed thousands of these procedures. 8. Where are facet joint injections performed? a. Facet joint injections are performed at our state of the art SNDC procedure suites.
Overview Hip osteoarthritis is a degenerative disease involving the cartilage in the hip joint. Osteoarthritis occurs when the protective cartilage surrounding the end of your bone begins to wear down over time. It can most commonly affect the knees, hips, hands, and spine. Symptoms can usually be managed but the damage to the joints can never be reversed. Risk factors for developing osteoarthritis include age, gender, obesity, previous joint injuries, repetitive stress on a joint, genetics, bone deformities, and metabolic disorders. Symptoms Symptoms of osteoarthritis develop slowly over time and can vary from person to person. Most commonly, patients will experience joint pain, stiffness (especially in the morning), tenderness around the joint, loss of flexibility or range of motion, grating sensation, and swelling. Diagnosis Diagnosis of osteoarthritis of a joint can be made with x-ray of the joint. MRI may also be useful in diagnosing osteoarthritis. Treatment Treatment of osteoarthritis first begins with lifestyle changes including consistent exercise and proper weight management. Physical therapy and pool therapy have also been shown to be effective in helping treat osteoarthritis pain. Additionally, alternative movement therapies such as tai-chi and yoga have been found to help reduce pain caused by osteoarthritis. Traditional medication options include acetaminophen (tylenol), and non-steroidal anti- inflammatory drugs (NSAIDs) such as ibuprofen, or aleve. Supplements such as glucosamine/chondroitin, capsaicin, and omega-3 fatty acids, while controversial in efficacy, have anecdotally reduced patient’s osteoarthritis pain. Typically, if lifestyle changes, therapies, and medications fail to relieve pain, then cortisone or steroid injections can be performed to help reduce inflammation in the hip joint. Finally, if all conservative measures fail the patient can undergo surgery to replace the hip joint. This is typically done by an orthopedic surgeon.

Piriformis syndrome occurs when the piriformis muscle, which is located deep in the buttock, causes pain. The piriformis muscle starts at the lower spine and attaches to the upper thigh bone. It functions to rotate the hip outward. What causes Piriformis Syndrome? Swelling, inflammation and spasm can occur in the piriformis muscle due to trauma, prolonged sitting or repetitive injury such as from sports. The pain may run down the back of the thigh. How is Piriformis Sydrome diagnosed? There is no direct, definitive test for Piriformis Syndrome. It is diagnosed by history and physical exam. Imaging may be ordered to rule out other pathologies. How is Piriformis Syndrome treated? Avoiding the activities that trigger the pain is important. Rest, ice, and heat can be helpful. Physical therapy, stretching, and exercises can also help relieve pain. Anti-inflammatories and muscle relaxers can ease pain. Injections with a steroid or botox can reduce the inflammation, pain, and spasm.